The researchers featured in the video, post-docs Jaehoon Choe and Matthew Phillips work for HRL Laboratories. Did they know the PR dept. was going to take their interviews and inject them with awesome graphics and all sorts of hyperbole? Is it marketing capitalizing on research, or research capitalizing on marketing?
I plan to dig deeper into this story and update as more info emerges and I get a better understanding of the study.
We’ve covered Dr. Adam Gazzaley director of the Gazzaley Lab at UCSF previously so I was excited to see he was being interviewed for one of my favorite podcasts, ShrinkrapRadio by Dr. David Van Nuys. I’m a big fan of Dr. Dave and have been enjoying his interviews with top psychologists for years. (Especially those with Jungian analysts.) I’ve clipped an excerpt of the interview that deals directly with tDCS and brain stimulation below but I highly recommend checking out the entire episode as it provides an excellent framework for understanding the notion of brain training using technology including video games designed specifically to enhance memory and cognition.
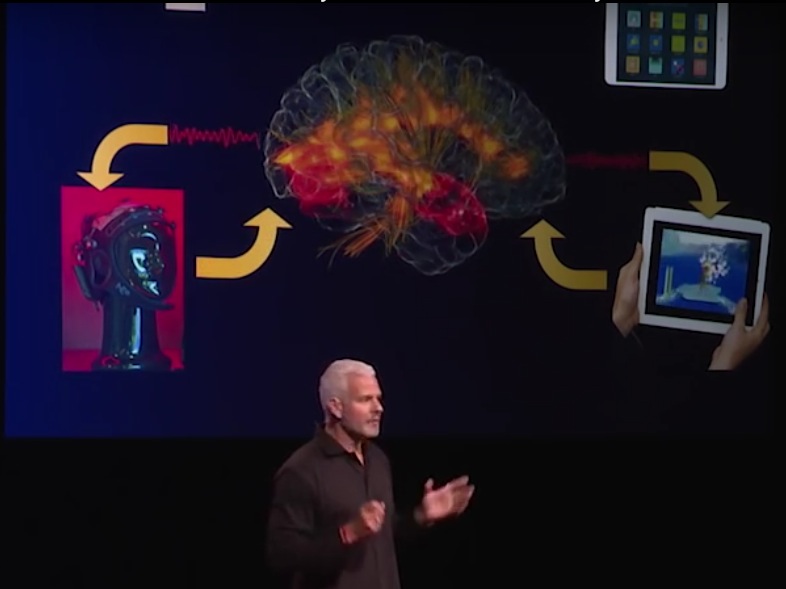
In this clip Dr. Gazzaley lays out what clearly is the near-future of non-invasive brain stimulation… You’re playing a video game that has been optimized to enhance working memory (for example). At the same time your EEG is being monitored for brain activity. According to the EEG data, tDCS (tACS, tRNS etc) is activated for the purpose of enhancing activity in that region of your brain. As your game accuracy increases, the game adapts to increase difficulty to an optimum training level. Loop!
Here’s a 2 minute clip from Dr. Dave’s interview with Adam Gazzaley
Dr. Shapiro’s company (he is the co-founder and non-executive director), Pure Tech Health created Tal Medical, to develop an LFMS treatment/device.
This is most likely the nexus for looking into LFMS in the first place:
The panel discusses TMS, which has recently been approved by the FDA for treatment of depression. But Dr. Shapiro goes on to discuss LFMS, which (to my readers anyway) is especially interesting because it uses so little power to achieve its effects. (As opposed to TMS which is too complicated and powerful to ever become part of the DIY community. Never say never!)
In 2013, Tal received initial proof-of-concept data from a randomized, double-blind, sham-controlled trial in patients with major depressive and bipolar disorders conducted by McLean Hospital, a leading psychiatric research hospital affiliated with Harvard Medical School. In the study, a single 20-minute treatment demonstrated rapid onset of action, substantial effect size, and a strong safety profile. Given this unique, rapid effect of LFMS treatment, the National Institute of Mental Health has selected LFMS for a multi-site clinical trial. The trial is examining the efficacy and durability of the treatment over an extended period of time in patients with major depressive disorder.
Researching possible patents led to Michael Rohan, Ph.D. and the Harvard Low Field Magnetic Stimulation Lab. I assume there is a partnership between the Harvard Lab, McLean Hospital and Tal Medical, though I could not find any formal announcement. Click through the lab link to do a deeper dive into ongoing research they are presently involved with, including clinical trials.
What is the most surprising or interesting research case you have worked on?
The findings where the data doesn’t show what you expected are always the ones that mean the most. In one study we were looking at the effect of gentle electrical stimulation (tDCS) on memory in healthy people; we compared sham (‘fake’) stimulation with a low and a high dose of tDCS. My hypothesis was that the higher the dose the better would be the performance and I couldn’t have been more wrong. The findings showed that the sham stimulation did nothing (as predicted), the low dose improved performance significantly, and the high dose behaved most similar to the sham stimulation.
This puzzled us so we brainstormed the findings and came back to the idea of homeostasis, where you can push the healthy brain a little but if you push it too much it will ‘push back’. Essentially, there are only limited gains in brain function that can be achieved in the healthy brain. That finding, which was from an Honours project, that I had initially worried was uninterpretable, resulted in a publication, two current PhD projects, and set me off on a different path with this aspect of my research.
Great example of exactly what we’re up against. The study in the previous post found no effect on Working Memory in older adults targeting dorsolateral prefrontal cortex (dlPFC). This study did find a positive effect on Episodic Memory in older adults targeting left lateral prefrontal cortex (PFC).
Episodic memory displays the largest degree of age-related decline, a process that is accelerated in pathological conditions like amnestic Mild Cognitive Impairment (aMCI) and Alzheimer’s Disease (AD). Previous studies have shown that the left lateral prefrontal cortex (PFC) contributes to the encoding of episodic memories along the life span. The aim of this randomized, double-blind, placebo-controlled study was to test the hypothesis that anodal tDCS over the left lateral PFC during the learning phase would enhance delayed recall of verbal episodic memories in elderly individuals. Older adults learned a list of words while receiving anodal or placebo (sham) tDCS. Memory recall was tested 48 hours and 1 month later. The results showed that anodal tDCS strengthened episodic memories, an effect indicated by enhanced delayed recall (48 hours) compared to placebo stimulation (Cohen’s d effect size=1.01). The observation that PFC-tDCS during learning can boost verbal episodic memory in the elderly opens up the possibility to design specific neurorehabilitation protocols targeted to conditions that affect episodic memory such as MCI.
Improved working memory is why many of us are interested in tDCS. Here’s another study showing no effect. Looks like a good study, though it’s a single-session of tDCS. Of late I’ve noticed more studies targeting working memory using the N-back test to measure. I’m hopeful a protocol will be discovered (i.e. a different montage, dosage, or perhaps tACS) that does improve working memory.
Transcranial direct current stimulation (tDCS) has been put forward as a non-pharmacological alternative for alleviating cognitive decline in old age. Although results have shown some promise, little is known about the optimal stimulation parameters for modulation in the cognitive domain. In this study, the effects of tDCS over the dorsolateral prefrontal cortex (dlPFC) on working memory performance were investigated in thirty older adults. An N-back task assessed working memory before, during and after anodal tDCS at a current strength of 1mA and 2mA, in addition to sham stimulation. The study used a single-blind, cross-over design. The results revealed no significant effect of tDCS on accuracy or response times during or after stimulation, for any of the current strengths. These results suggest that a single session of tDCS over the dlPFC is unlikely to improve working memory, as assessed by an N-back task, in old age.
[Did you just pop back for the Caputron promo code? It’s ‘diytdcs’ without the quotes.]
Robin Azzam is the founder of Caputron. While pursuing a Masters in medical engineering at New York City College, Robin realized there was a need in the research community for a place to source brain stimulation supplies. Shortly after leaving a position in product development at Soterix Medical, Robin and a few friends set up Caputron with the intention of becoming a ‘one stop shop’ for all things related to brain stimulation. His time at Soterix, working alongside Marom Bikson, led to the sort of relationships that allowed Caputron to become a distributor for high-end products like Soterix HD-tDCS and Neurosoft’s TMS devices. But Caputron also began to carry a large selection of electrodes, cables, straps and stimulation-related accessories. Caputron is now developing their own products, and hope to have their own research-grade home DC current device on the market by the end of the year. They recently began selling their mindGear device which I will cover in detail in the near future.
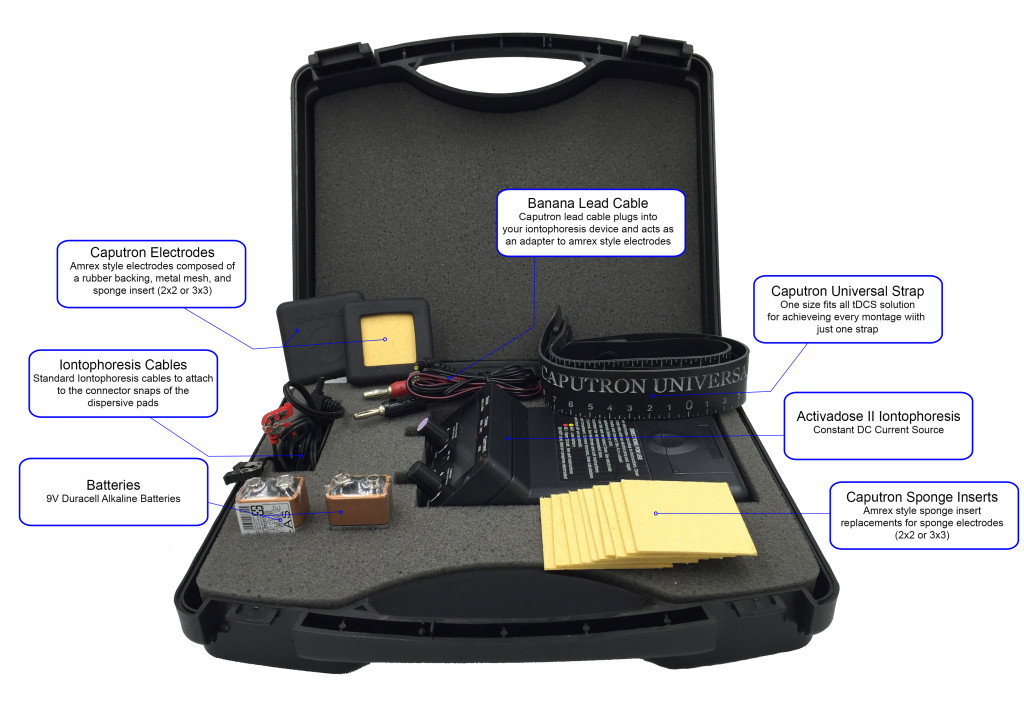
What DIYtDCS readers will likely find most exciting is Caputron’s ActivaDose II Starter Kit. This is the FDA cleared iontopheresis device widely used ‘off label’ for tDCS. It is the device used by two of my previous podcast guests, Dr. Jim Fugedy (for treating depression) and, (at the time) Michael Weisend for research. But Caputron has customized the included accessory package making it tDCS-friendly right out of the box.
In the three years I’ve been running the blog I’ve not previously felt comfortable recommending any specific tDCS device (mostly due to my own ignorance of electronics). I’ve either had doubts about the device itself or not had confidence in the vendor’s customer support. But based on my own experience with the ActivaDose products, the fact that it’s an ‘FDA cleared’ device, and also that it’s coming from Robin and his team, I feel, finally, that we have a product/vendor you could recommend your Mother to. (Assuming she does her homework!)
To that extent, I asked for, and Robin agreed to, a discount on all Caputron products for DIYtDCS readers. Simply plug the promo code ‘diytdcs’ (without quotation marks) into the Voucher window at checkout for a generous discount.
Here’s our interview. Your feedback is welcomed!
Note: The ActivaDose II has a max output of 4.0 mA which, as you know if you’ve done your homework, is twice as much as is typically used in tDCS research.
Many of the leading tDCS researchers contribute to this Open Access article on clinical application of transcranial electrical stimulation (tES) techniques. Read it online, or download the pdf. (HatTip to Reddit user gi67)
Last month, the FDA held a public workshop on this topic. (I spoke on one of the panels, though I have no financial interests in these products.) Based on the discussion paper released ahead of the workshop, it seems that the agency intends to regulate these devices—it just hasn’t quite figured out how to do so. But although the FDA may have the expertise to regulate these devices, the idiosyncrasies of medical device law—namely, the complications regarding “intended use” claims—may not make this the best option, especially given the recent entrance to the market of devices that make no claims at all and instead bill themselves as “direct current sources.” The situation may require a novel solution—such as collaboration between the FDA and CPSC or the involvement of a third party, such as the National Academy of Medicine—to ensure the construction of a coherent framework that best encompasses devices on the market now and anticipates the complex issues that may arise in the future.
Update 12/16/2015: Bouncing this story up to the top again today because of news of a new study that links Autism to SSRI (anti-depressant) use in pregnant women.
The analysis also found that women who were prescribed more than one class of antidepressants during the last six months of pregnancy were more than four times more likely to have a child with autism, compared with women who did not take antidepressants while pregnant.
Update 10/16/2015: Today I learned that this study is ongoing and recruiting participants. If you or someone you know is pregnant and dealing with severe depression, consider contacting study author Simone Vigod at Women’s College Hospital in Toronto. Study Protocol. You can also follow Simone on Twitter.
Tatania Samburova, a Russia-born economist who immigrated to Canada two years ago, developed depression before becoming pregnant. Her depression left her feeling hollow, even suicidal.
“You do not feel yourself living. You do not want anything, you do not want to go somewhere, to do something,” she said.
Her doctor offered her antidepressants, but, while she knew they would offer her relief, she decided against using them over fears they may harm her child.
“Even if it will bring me, right now, some kind of relief, it can also affect the life of a little child,” she said.
Instead, she travelled to Mount Sinai (hospital) every day for three weeks to be treated as part of the study. She doesn’t know for sure if she received a sham treatment or the actual tDCT stimulation but suspects she had the actual therapy because within days her appetite returned and she felt her mood lifting.
“This treatment brought happiness back to me; it brought life back to me,” she said.
She remains well today, with her baby due mid-March.
Vigod notes that some women are so desperate for treatment that they are not waiting for the study results.
“I can tell you anecdotally that women are buying devices like this in the U.S. and using them at home, but they haven’t really been tested to see if it works to make the depression better.”
From the study protocol: The active tDCS intervention is active 2 mA tDCS. Direct current is transferred continuously for 30 minutes with a pair of saline-soaked sponge electrodes (contact area of 5 × 7 cm), and delivered by a specially developed, battery-driven constant current stimulator. The electrodes are placed over F3 and F4 according to the 10–20 international system for electroencephalogram placement.
Lifehacker UK spoke with Nick Davis, a lecturer in psychology at Swansea University. We began by asking whether there is any actual evidence that tDCS can have a beneficial effect on its users:
There is relatively little evidence at the moment that tDCS can lead to improvement in real-world activities. The closest we have got so far is in military contexts like spotting threats such as snipers. Researchers have used immersive video games to train soldiers to respond when they see something that might be a threat – tDCS seems to make people a little better.
With regards to the potential dangers of using these devices outside of a proper clinical environment, Davis continued:
In my lab, the major concern I have is that I might trigger a seizure. A seizure results from over-excitable brain circuits, so adding more excitability with tDCS could be dangerous. I would not allow anyone to take part in my experiments if they have a family history of epilepsy, or if they have had excessive amounts of drink or drugs in the day before the experiment as these are also risk factors.
I am also worried that younger people, whose brains is still developing, might also be using tDCS without proper supervision. There are too many unknown factors in how tDCS affects the brain for it to be safe for unsupervised use, and I think we should be very cautious even in research labs.
Update 3/1/17 Not sure when it happened, but a reader alerted me to the fact the tDCS Shield addon was abandoned.
After many conversations with experts in the field of neuroscience and brain-computer interfacing, we have made the difficult decision to discontinue development of the tDCS Shield.
Very interesting! A successful ‘maker’ lab with previous EEG device success (32 channel, research-level EEG device) embarks on a lower cost, 4 channel EEG-device-for-the-masses Kickstarter campaign. It’s hugely successful, and fully funded ($80k) with 30 days left to go. So they launch a ‘stretch goal’ for an additional $80k of funding to add the option to pre-order (for $50) a tDCS module.
What does this mean for you and I? Well, it at least certainly points to the possibility that within the next few years we could be sitting in front of a computer screen, monitoring our EEG output (brainwaves, more or less) while we try out a tDCS (tACS, tRNS, tPCS etc.) montage. As in, “Oh Interesting! 1.5 mA stimulation to DLPFC (your forehead) tunes my Theta into that zone that makes me feel like writing a song!” (Kidding but you get the idea).
This gets me really excited when I think about the possibility of thousands of us doing it and contributing the collective data in a useful way to scientific research.
This is what first caught my eye! 3d printed HD-tDCS electrodes?
At OpenBCI, we are cautiously optimistic about the beneficial potential of transcranial direct-current stimulation (tDCS). As always, safety is our number one priority. We hope to educate the public about proper tDCS techniques, and to offer a new, open-source platform for studying the effects of tDCS on electrical brain activity. If we hit the $160,000 stretch goal, we will provide the option to pre-order a tDCS Shield that is compatible with both the Ganglion and our 32bit board. In addition, we will design custom Ultracortex node mounts for tDCS-specific electrodes. Anybody with the complete Ganglion+Ultracortex+tDCS system will be able to perform simultaneous neurostimulation and neurorecording, trying out different electrode configurations and creating custom “closed-loop” brain-computer interface systems.
tDCS is a type of neurostimulation in which a low-amperage direct current is passed through the scalp from a positively charged electrode (anode) to a negatively charged electrode (cathode). Some research has claimed that tDCS can increase cognitive performance and assist in the treatment of cognitive disorders such as depression and ADHD. Other studies have reported that there is no statistically conclusive evidence that tDCS has any net cognitive effect. Despite the effects of tDCS being critically debated, it is widely accepted that tDCS—when adhering to safety protocols and done in a controlled manner—is a safe method of brain stimulation.
Spread the word, and help us double our goal!
Joel testing a breadboarded prototype of the tDCS Shield: “Ooooo! It’s tingly…”
From an older post, but I found it in a tweet from Halo Neuroscience‘s Senior iOS engineer, Rich Lowenberg @richlowenberg. We met Halo Neuroscience back in May, 2014. My sense is we may be hearing more from them soon (though it’s just a hunch based on recent media mentions). If you’re in the San Francisco area, they are recruiting for a TES (transcranial electric stimulation) ‘Hand Strength Study‘.
Halo Neuroscience is working on technology to “boost brain function” and “[elevate] cognitive performance” via headband. Speaking to TechCrunch, Halo co-founder Amol Sarva explained that the company’s tech is being developed to offer not just a remedy but also an edge, as it “stimulates brain function in [both] sick people and healthy people.” He continued:
It makes the brain work better—a wide range of potential effects from accelerating learning to improving body movement control […The] field is a big new area—not just sensing things in the brain or ‘reading’ it, but sending waves into the brain and ‘writing’ to it […] Nobody believed it was real! We didn’t either. Until we tried it.
Halo uses a version of the popular transcranial direct-current stimulation (tDCS) method, which involves “priming” or “inhibiting” brain cells’ firing patterns by sending low levels of electricity through electrodes in certain scalp areas. This makes particular brain cells more or less likely to fire, therefore targeting brain activity toward certain performance standards.
Note that I do have a relationship with Caputron. When you make a purchase from their site using promo code diytdcs (add to ‘voucher’ box, any item on their site) you receive a discount and I receive an equivalent amount in exchange for providing them a visitor. I have been offered similar relationships with various vendors, but Caputron was the first I felt comfortable partnering with, primarily because their customer support and communication has been outstanding. But also because they carry the ActivaDose Iontophoresis Device which is an FDA approved device (approved for iontophoresis, not tDCS, but the point is that the components and quality are medical grade.) Bundled with the Caputron electrode kit, this is an excellent choice for anyone looking to experiment with tDCS. This is the only device I am personally recommending at this time.
That said, Caputron has just started carrying other DIY DTC (Direct To Consumer) tDCS devices. They announced yesterday that they now carry Super Specific Devices tDCS Stimulator
Caputron is rapidly becoming the primary distributor of all things brain stimulation. This puts them in the unique position of being able to bundle appropriate electrodes and cables with the various devices they carry.
But Caputron are also manufacturers and we can look forward to interesting tDCS related products of their own coming soon.
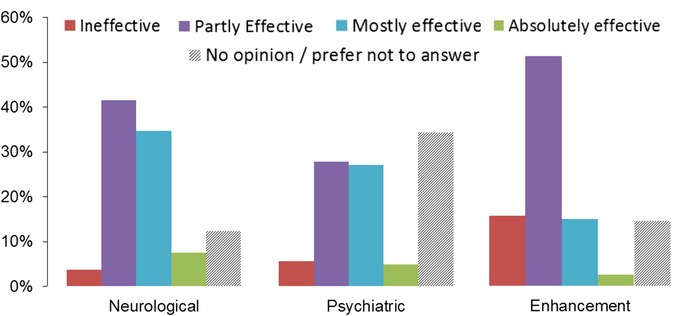
Researchers’ assessment of the efficacy of tDCS in clinical and enhancement contexts. Data represents distribution of responses (%) for each category, see legend.
The cautious approach to use of tDCS is also reflected in the low ratings for efficacy of its use to enhance normal functions. The tDCS research community appears well aware of current limitations and the need for future research to address those. The appearance of enthusiastic articles in the media and online suggest that these cautious views are frequently not being communicated clearly to the public. Researchers must make their views about the limited evidence of safety and efficacy clearly when speaking with the media or communicating with the public.